
OPEN ENROLLMENT MAY BE OVER BUT!
Over 90% of our clients qualify for enrollment into a free/reduced cost plan at ANY TIME OF THE YEAR due to a special enrollment qualification based on your income!
If your income for you/your family size falls within the ranges below,
you can qualify for a $0 Health-Plan for 2025!
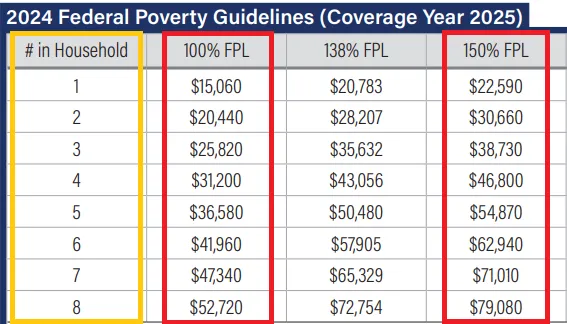
(Not all carriers are shown below)
Current Contracted Carriers
(Not all carriers are shown below)

Current States We Service

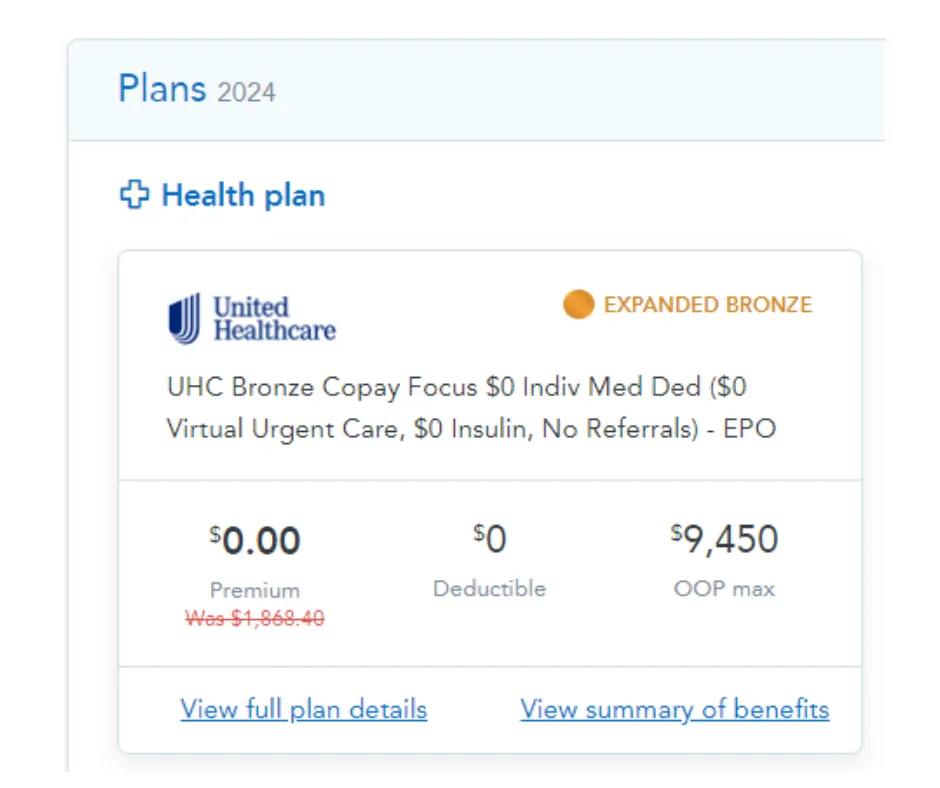
Previous Client's Insurance Examples!
(Plans shown below may not be available in your exact state/zip code)
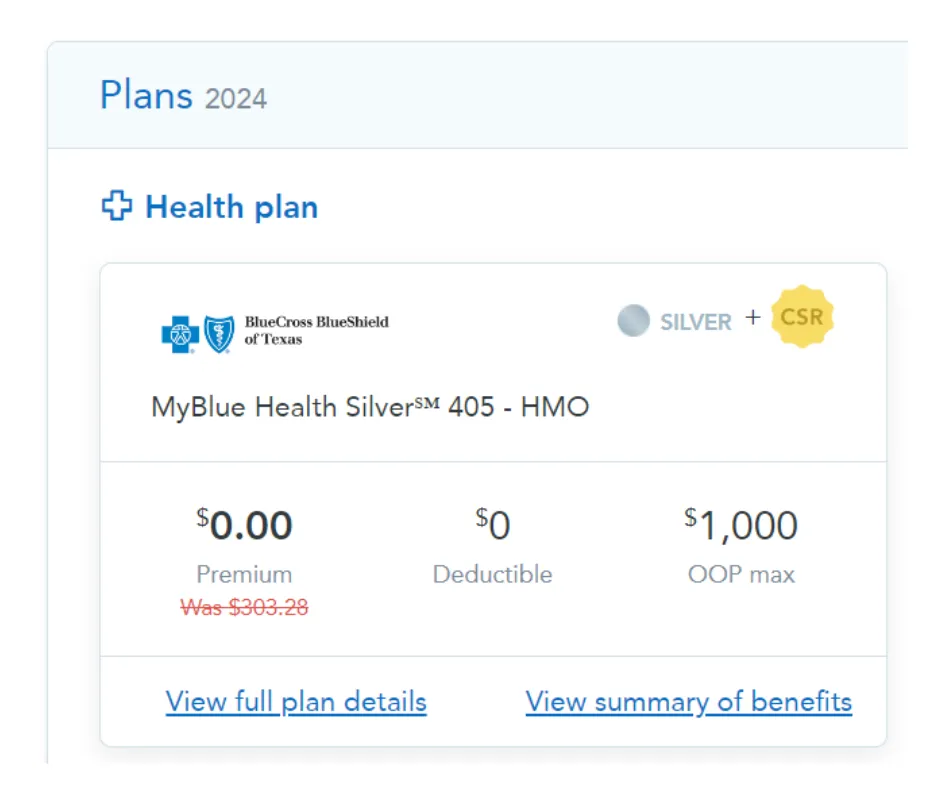
Texas, 78521 Zip Code
2 Person Household
$21,900/Yr Annual Household Income
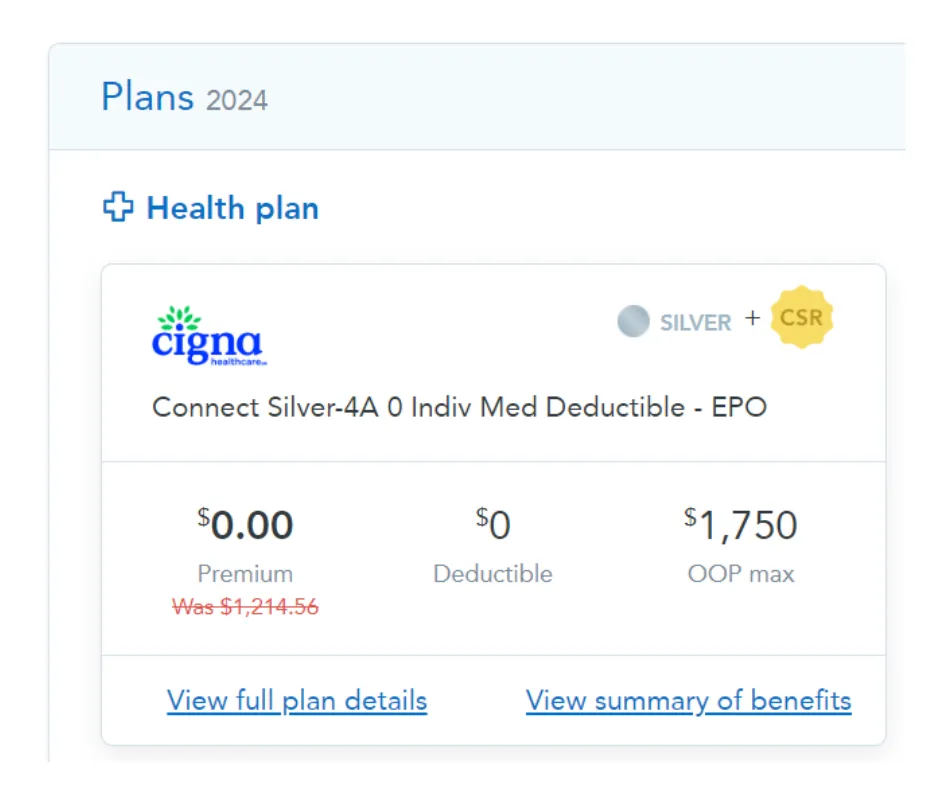
Tennessee, 38357 Zip Code
1 Person Household
$19,800/Yr Annual Household Income
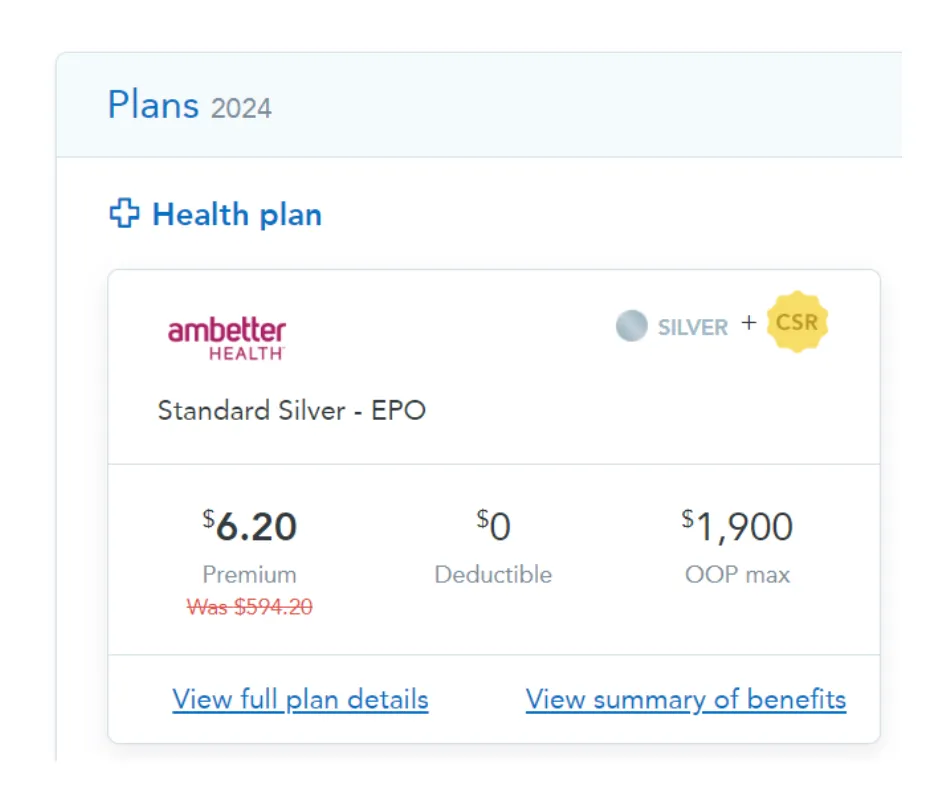
Louisiana, 70062 Zip Code
1 Person Household
$21,200/Yr Annual Household Income
Louisiana, 70517 Zip Code
2 Person Household
$43,000/Yr Annual Household Income
Some of Our Happiest Customers!
Over 3,000 clients served in the last year!

Maria G. - Phoenix, AZ
"Before, none of my prescriptions were covered, and my premium was sky-high. Thanks to applying here, I finally have affordable care and my medications are covered! "
⭐⭐⭐⭐⭐
James L. - Dallas, TX
"I was stuck paying outrageous premiums with doctors that weren't even in my network. After applying, not only did I get a FREE plan, but my doctor visits are covered again!"
⭐⭐⭐⭐

Lynn P. - Orlando, FL
"My family struggled with high premiums and uncovered prescriptions. After finding this site, our insurance finally fits our budget and healthcare needs. Highly recommend Adroit!"
⭐⭐⭐⭐⭐

Karen M. - Charlotte, NC
"I was hesitant to switch plans, but after applying through this site, I found an affordable plan that covers my specialist visits! Plus I was able to enroll without speaking on the phone, pretty cool!"
⭐⭐⭐⭐

Robert D. - Phoenix, AZ
"I used to pay way too much out-of-pocket for my claims. Now, with better coverage, I'm saving so much money! Thank you Adroit!"
⭐⭐⭐⭐⭐

Steven H. - Houston, TX
"The process was super easy, and I found a plan that included my preferred doctors. I usually don't click on online ads, but I'm glad I did for this one."
⭐⭐⭐⭐⭐

Copyright 2026 . All rights reserved
Privacy Policy
Data Collection: Our Agents collect Personally Identifiable Information (PII) solely for the purposes mentioned in our Comprehensive Attestation Agreement.
Data Protection: We are committed to ensuring the privacy and safety of your PII. Your data will not be shared for any purposes other than those explicitly stated in our agreement.
Income Attestation: We use your income information solely to determine eligibility for health insurance programs and potential subsidies.
Terms of Service
By using our services, you agree to the following terms:
Representation: You grant the authorized agent, as mentioned in the attestation disclaimer, the authority to act on your behalf concerning health insurance matters, including enrollment, renewals, and related decisions.
Accuracy: You confirm that all information provided is true and accurate. False or misleading information can lead to the termination of services.
Revocation: Your consent remains in effect until you revoke it. You may revoke or modify your consent at any time.
Limitation of Liability: The authorized agent and associated entities are not liable for any errors or omissions in the services provided or for any damages, including indirect or consequential damages.
TCPA Disclaimer
By providing your phone number, you expressly consent to receive auto-dialed and/or pre-recorded telemarketing calls, text messages, and/or emails from the authorized agent mentioned in the attestation disclaimer at the phone number and email address you provided, including for marketing purposes.
You understand that consent is not a condition of purchase.
Message and data rates may apply.